18 yr old female, with , fever, vomitings and loose stools.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.”
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CASE:
18 yr old female, Agricultural labourer by occupation ,brought to the casualty with chief compliants of
fever since 4 days, vomitings since 3 days,
loose motions since 1 day.
C/O shortness of breath since morning.
Her resp. Rate : 24 cpm and spo2 93%@RA.
HOPI:-
Patient was apparently asymptomatic 4 days back, then she developed fever - high grade associated with chills , rigors and headache, not associated with cold , cough.
Vomitings--
10 to 12 episodes, watery in consistency,non- bilious non-projectile,since 1 day , associated with decreased Appetite.
Stools--
5-6 episodes since 1 day ,watery in consistency, no blood or mucus in stools.
Past history:-
Not a known case of DM, HTN, Epilepsy, TB.
On examination;-
Patient was conscious, coherent, cooperative, moderately built and moderately nourished.
No pallor, icterus, cyanosis, clubbing, generalised lymphadenopathy, edema.
Vitals:-
Temp:- 98.5 F
Bp:- 90/60 mm hg
PR :- 110 bpm
RR:- 24 cpm
Grbs:- 119 gm/dl
Spo2 : 85% @ RA
Cvs:- S1, S2 heard .
RS:- BAE present, nvbs.
P/A:-soft, non-tender.
CNS:- HMF intact.
Provisional diagnosis:-
Fever with multiorgan dysfunction.
? Viral pneumonia.
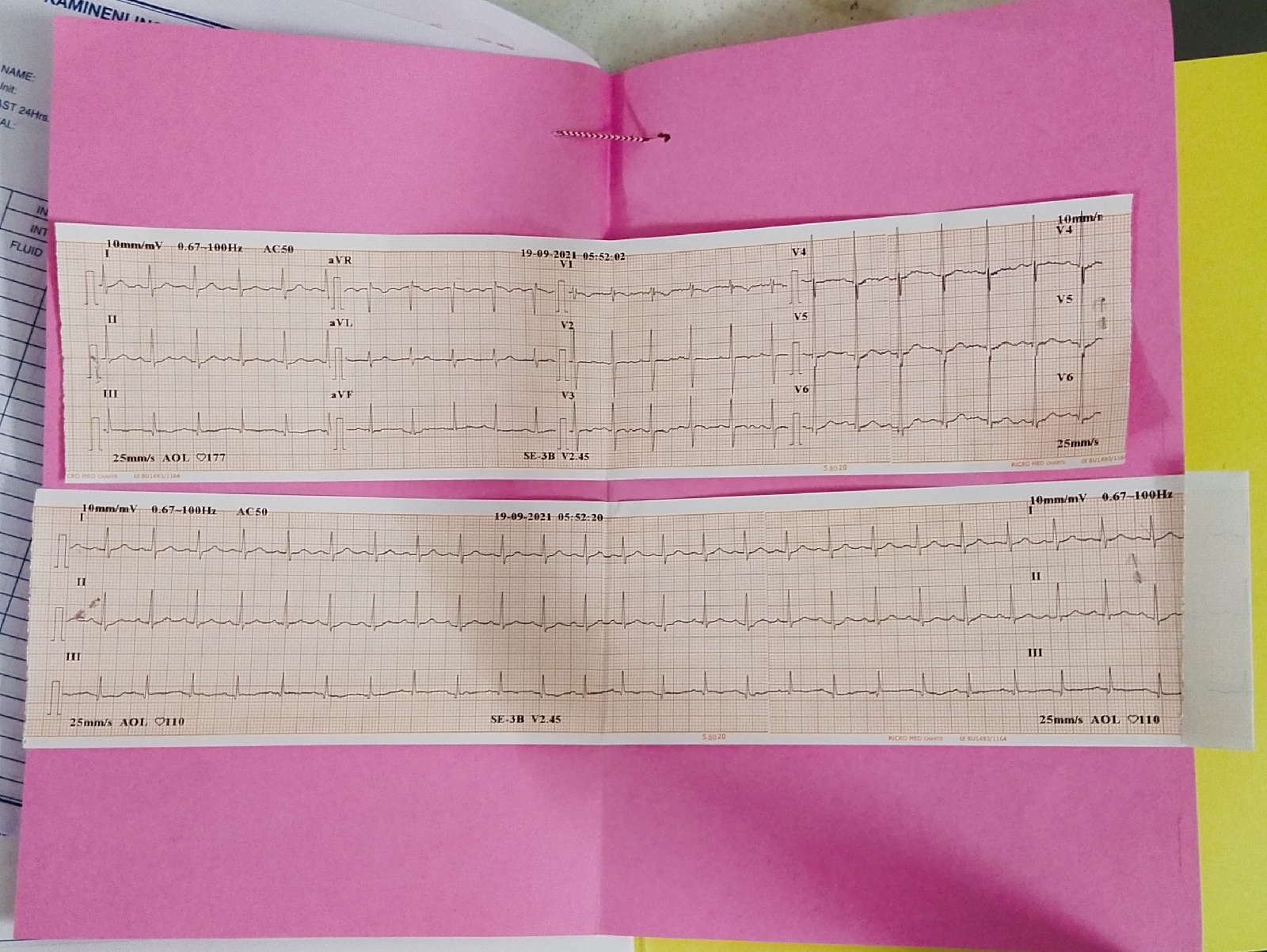
ECG:-
Fever chart




Ultrasound:-
 Chest x- ray :-
Chest x- ray :-

HRCT chest:-



Treatment:-
1. IVF :NS,RL @150 ml/hr
2. Inj. Pantop 40 mg IV/OD
3. Inj. Zofer 4 mg IV/OD
4.Inj.Neomol 100ml IV/sos (if temp>101F)
5. Tab.Pcm 500 mg po/tid
6.Cap. doxycycline 100 mg po/bd
7. Tab. Azithromycin 500 mg po/od.
8. Temp, BP, I/O charting.
SOAP 20/09/2021.
S-
Patient complains of
SOB
Cough with sputum
Fever
O-
Patient was c/c/c
Afebrile,
Bp: 100/60 mm hg
PR: 120 bpm
RR:- 38 cpm
Cvs: S1, S2 present
Rs: BAE present, nvbs
P/A:- soft, non - tender.
CNS:-HMF Intact.
A-
Viral pneumonia with thrombocytopenia, with multiorgan dysfunction.
P-
1.IVF :NS,RL @150 ml/hr
2. Inj. Pantop 40 mg IV/OD
3. Inj. Zofer 4 mg IV/OD
4.Inj.Neomol 100ml IV/sos (if temp>101F)
5. Tab.Pcm 500 mg po/tid
6.Cap. doxycycline 100 mg po/bd
7. Tab. Azithromycin 500 mg po/od.
8. Temp, BP, I/O charting.
9. Inj. NA double standard ( 2 amp in 36ml of NS) @ 2 ml/ hr.
10. Syp. Ascoril 15 ml po/tid.
Course in the hospital:-
18 yr old female came to the casualty with c/o loose stools, vomitings and SOB (grade 4).
On presentation- patient was tachypnic, febrile with sepsis, RR 38cpm, spo2 85% at RA 99% at 10lit of O2.
Platelet count-46000, with derranged LFT and RFT with HRCT showing --
Numerous centrilobular nodules many of them are having tree in bud configuration in both the lungs involving all lobes --
F/S/O endobronchial infection.
Corads -2.
On day 2 --
Spo2- 83%@ RA and 99% with 10L of O2.
Patient was referred to higher centre in view of covid suspect.
Comments
Post a Comment