A 50 yr old male with pain abdomen
This is an online E log book to discuss our patient\"s de -identified health data shared after taking his/her/guardian\"s signed informed consent. Here we discuss our individual patient\"s problems through series of inputs from available global online community of experts with an aim to solve those patient\"s clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs in the log.

Cheif complaints:-
A 50 yr old patient came to the casuality with chief complaints of pain abdomen since one day.
History of present illness:-
8yrs back patient had c/o polyuria when he was diagnosed with DM and,
5yrs ago diagnosed with HTN when he went for regular check up for his Diabetes.
3yrs ago pt had pain abdomen after alcohol intake when he was given ryles aspiration and IV fluids ..? Pancreatitis.
1 year ago..
He was admitted in our hospital because of his uncontrolled Sugars, with non proliferative diabetic retinopathy, right side diabetic foot with post Gilles amputation. Patient underwent forefoot amputation 10 months ago.
At the time of discharge 1yr ago patient was adviced to use inj human mixtard twice daily.but pt was non compliant to insulin and is using mixtard as OD dose since 6months.
chronic alcoholic since 20 yrs .
Now..
Patient came with pain abdomen in the epigastrium and umbilical region since 1day, which was sudden in onset, gradual in progression, squeezing type , with no aggrevating and relieving factors.
Patient has no history of vomitings, loose stools , and fever.
No h/ o constipation.
H/ o alcohol intake 2 days ago.
Past history:-
Not a k/c/o asthma, TB,epilepsy.
Personal history:-
Patient takes mixed diet, his appetite is normal, sleep is adequate, Bowel and bladder movements are normal.
He is a chronic alcoholic since 20 yrs.
Family history:-
No significant family history
General examination:-
Patient is conscious coherent cooperative, moderately built and moderately nourished.
No pallor, icterus, cyanosis, clubbing, lymphadenopathy.
Systemic examination:-
Cvs:-
S1 S2 heard, no murmurs
Rs:-
BAE - present, Nvbs
Per abdomen:-
Soft and tenderness present in epigastric , umbilical and left lnguinal region.
CNS:- normal.
Vitals:-
Temp -98.7 F
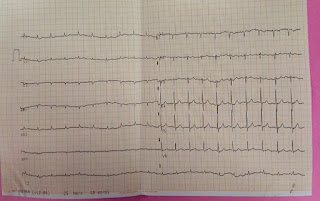
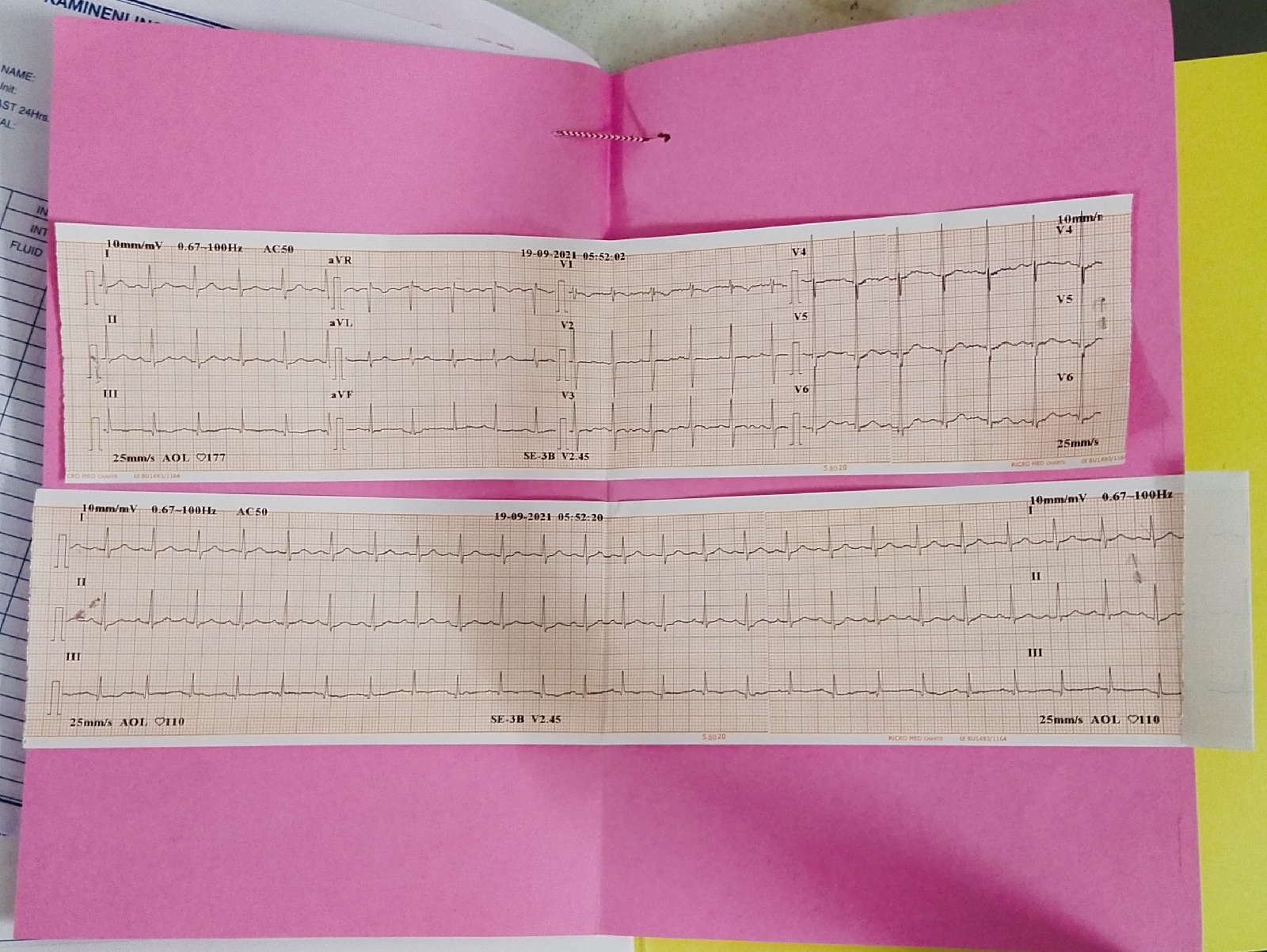
PR:- 102bpm
RR:-18 cpm
BP:- 120/70 mm of hg
Grbs:- 451
Provisional diagnosis:-
? Acute pancreatitis
? Alcoholic gastritis
K/c/o DM type 2 .
Investigations:-











Treatment:-
1. IV fluids
2. Inj. tramadol
3. Inj. Pan
4. Inj. Zofer
Discharge summary:-
Discharge Date
Date:23/06/201
Ward:GM
Unit:5
Name of Treating Faculty
DR. ARJUN
DR.HAREEEN
DR. VAISHNAVI (PGY2)
DR. CHANDANA (PGY1)
DR.KRUPA(INTERN )
DR.NIKITHA( INTERN)
DR. SRAVANI( INTERN)
DR.THEJASWINI (INTERN)
DR.RAMYA(INTERN)
Diagnosis
Acute pancreatitis with uncontrolled sugars
Case History and Clinical Findings
chief complaints:-
A 50 yr old male patient came to the casuality with chief complaints of pain abdomen since one day.
History of present ilness;-
8 yrs back patient had complaints of polyuria when he was diagnosed with diabetes mellitus and ,
5 yrs ago diagnosed with hypertension when he went for general checkup for his diabetes .
3 yrs ago patient had pain abdomen ahter intake of alcohol and was given ryles aspiration and iv
fluids.... ? pancreatitis.
1 yr ago , he was admitted in our hospital because of his uncontrolled sugars , with non proliferative
diabetic retinopathy , and right side diabetic foot with post gilles amputation . patient underwent
forefoot amputation 10 months ago. At the time of discharge , patient eas advised to use inj. human
mixtard twice daily but pstient was non compliant to insulin and is using mixtard as OD dose.
he is a chronic alcoholic since 20 yrs.
Now , patient developed pain abdomen in the epigastric and umbilical area , which was insidious in
onset , gradual in progression, sqeezing type of pain , with no aggrevating and relieving factors.
patient has h/o alcohol intake one day before he came to the hospital.
No h/o vomitings, loose stools, and fever .
No h/o constipation .
past history;-
no h/o asthma,TB, epilepsy.
general examination;-
patient was conscious,coherent,cooperative moderately built and moderately nourshed.
No pallor, icterus, cyanosis, clubbing, lymphadenopathy.
patient underwent forefoot amputation 10 months ago.
systemic examination;
cvs;-
s1 s2 heard, no murmurs
rs:
BAE +,
cns;- intact
Course in the hospital:-
Patient was admitted with pain abdomen since 1 week and vomiting 1 episode.
Secondary to the non compliance patient was kept on NBM for 1 day and slowly started on liquid diet and later solid diet.
Supportive management with IV fluids , inj. Tramadol ( for pain abdomen), pan, zofer ( for vomiting)given.
His pain abdomen subsided on day 3 of admission .
He was given a trial of oral glimiperide or his uncontrolled sugars but his sugar were not on control, so restarted on insulin.
Psychiatric referral was taken in view of alcoholic dependence. They have advised for Liofen 20 mg bd( as anticraving drug), t. Benfomet , tab. Lorazepam.
Investigations:-
Serum amylase -111
Serum lypase -256
Name Value Range Name Value Range
COMPLETE BLOOD PICTURE (CBP) 20-06-2021 11:42:AM
HAEMOGLOBIN 15.0 gm/dl 17.0-13.0 gm/dl
TOTAL COUNT 7400 cells/cumm 10000-4000
cells/cumm
NEUTROPHILS 65 % 80-40 %
LYMPHOCYTES 26 % 40-20 %
EOSINOPHILS 04 % 6-1 %
MONOCYTES 05 % 10-2 %
BASOPHILS 00 % 2-0 %
PLATELET COUNT 2.16
SMEAR Normocytic
normochromic
ABG 20-06-2021 12:19:PM
PH 7.40
PCO2 35.8
PO2 107
HCO3 21.8
St.HCO3 22.9
BEB -1.8
BEecf -2.2
TCO2 41.6
O2 Sat 96.4
O2 Count 22.3
SERUM
CREATININE 20-06-
2021 01:45:PM
1.3 mg/dl 1.3-0.9 mg/dl
Treatment Given(Enter only Generic Name)
1. nbm till further orders.
2.inj. pan 40 mg iv od
3. inj.zofer 4 mg iv bd
4.inj. tramadol 10 amp in 100 ml ns iv sos
5.grbs 6 hrly
6.inj.human actrapid insulin s.c tid
7. ivf
8. moniter vitals
Advice at Discharge
1.tab. benfomet half tablet qid 1 month
2, tab. human mixtard 10 units s.c BD
3. inj. human actrapid s.c 10 units 2pm
4. tab, neuroben po od 1 month
5. alcohol abstinence.
Follow Up
review with fbs, plbs, hba1c, after 15 days
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR
ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact:
08682279999 For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed
and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been
explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY

Comments
Post a Comment