June Assessment

Please go through one particular answer of ten students in this link:
https://generalmedicinedepartment.blogspot.com/2021/06/bimonthly-formative-and-summative_19.html?m=1
and share your peer review of each answer with your quantitative marking input as well as qualitative insights into what was good or bad about the answer.
1. PULMONOLOGY
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
1) Evolution of symptamatology
20yrs ago- 1st attack of shortness of breath
From then, every year in January, episode lasts for a week
12yrs ago- admitted to hospital with severe shortness of breath
Current episode:
Started 30 days back, dyspnoea on exertion, relieved on rest,
But since 2 days, dyspnoea even at rest
Possible explanation: attacks of dyspnoea can be triggered by winter season, vegetative matter, dust, pollen ( provided dyspnoea occurred at the time of working in rice fields)
Possible etiology: vegetative dust (RICE)
On investigation: upon CT, lower airway problem is seen
Other associated symptoms :
1. Pedal edema since 15 days up till ankle level
2. Facial puffiness since 15 days
MY OPINION AND ANALYSIS:-chief complaints:-
Being SOB,facial puffiness and pedal edema
TO RULE OUT CARDIAC CAUSE OR RENAL CAUSE
As investigations and clinical examination show
BRONCHIECTASIS
AND ACUTE EXACERBATION OF COPD..
Im convinced with her analysis and review
Question 2-4:
Patient centered data
captured by students from 2016 batch in the link below:
MULTISYSTEM:
https://nikithaedam48.blogspot.com/2021/06/18-year-old-malefrom-miryalagudawho-is.html?m=1
CNS :
https://pallavi191.blogspot.com/2021/06/gm-cases.html?m=1
Renal :
https://61tejarshini.blogspot.com/2021/06/general-medicine-case-discussion.html?m=1
Captured by one student from 2017 batch in the link below :
CVS :
https://60shirisha.blogspot.com/2021/06/medicine-case-discussion_14.html?m=1
Captured by one student from 2019 batch in the link below :
Abdominal :
https://casescape.blogspot.com/2021/06/acute-kidney-injury-secondary-to.html?m=1
MY ANALYSIS OF THE FOLLOWING CASES:-
1.https://casescape.blogspot.com/2021/06/acute-kidney-injury-secondary-to.html?m=1
Overview:-
pt is diagnosed with AKI SECONDARY TO UROSPESIS
IN 2019
Came with similar complaints in june 2021
Could probably be a case of AKI ON CKD
RATHER THAN AKI
APPRAISAL:-GOOD CHARTING OF TRENDS OF SERUM CREATININE AND TLC COUNTS
NEGATIVE POINTS:-
COULD HAVE SHARED DEINDENTIFIED IMAGES OF THE PATIENT SO AS TO GIVE A CLEAR AND DETAILED OPINION ABOUT EXAMINATION
COULD HAVE SHARED A MORE DETAILED HISTORY OF HER HISTORY AFTER DIALYSIS SESSIONS FROM 2019 to 2021
FEVER CHART SHOULD HAVE BEEN SHARED
ANALYSIS:-THIS COULD BE AKI ON CKD
RATHER THAN AKI ALONE
2. CNS :
https://pallavi191.blogspot.com/2021/06/gm-cases.html?m=1
OVERVIEW:-
chief complaints of sudden fall followed by weakness of both the lower limbs (paraplegia) and loss of hand grip 10 days back, associated with bowel and bladder incontinence.
He is a known case of TB since 1month and on ATT - HRZE
Probably could be pott’s spine secondary to TB
APPRAISAL:-
Well
Presented case with detailed info about patient and imaging reports
NEGATIVES:-
Fever chart should have been shared and SOAP format of patients everyday progress
ANALYSIS:-Quadreparesis secondary to infectious spondylitis of C4, C5, C6, C7 and D1 with Epidural abscess at C5 - C6 level.
Clinically CNS:
Speech - normal
No signs of meningeal irritation
Right. Left
Tone. UL. N. N
LL increased. Increased
Power UL. 4/5. 4/5
LL. 1/5. 1/5
Cranial.nerves. : Intact
Sensory system : normal
Reflexes:
Right. Left
Biceps. 3+. 3+
Triceps. 3+. 3+
Supinator. 2+. 2+
Knee. 3+. 3+
Ankle. 3+. 3+
Plantar: extensor
I dont these findings actually are supportive of the daignosis
Because in a case of quadriparesis
The examination findings donot correspond
3. Renal :
https://61tejarshini.blogspot.com/2021/06/general-medicine-case-discussion.html?m=1
OVERVIEW:-Complaint of Altered Sensorium (Hypo active):It's since Morning,lethargy.
History of fever 10 days back,lasted for 3 days,(Outside Creatinine ?11-14.8)
Followed by Pedal edema with Anasarca with Shortness of breath present even at rest .
(Outside Creatinine reports 11)
He is a known case HYPERTENSION:5 YEARS and on T.STAMLOBETA OD.
He is also a known case of CHRONIC KIDNEY DISEASE:5 YEARS and on Conservative Treatment
(Outside Creatinine =? 3.2 mg/dl,5years back).
Present creatinine of 20mg/dl and previous baseline creatinine above normal
It is a case of AKI ON CKD with Level of consciousness:Drowsy but Arousable (Hypoactive, delayed response to commands).
Signs of meningeal irritation:No neck stiffness,no kerning's sign.
Higher mental functions: Intact
Reflexes: Present.
Suggestive of UREMIC ENCEPHALOPATHY (since urea levels being 340mg/dl)
NEGATIVES:-could have shared more clinical
Images (deidentified)
And fever chart should have been shared
Recent trends of RFT could have been shared
APPRAISAL:-Good presentation of the case with proper history and treatment plan
ANALYSIS:-
Since baseline creatinine levels are above normal
And current compliants of anasarca
With raised creatinine of 20mg/dl and urea of 340mg/dl
With a drowsy state suggests AKI ON CKD WITH UREMIC ENCEPHALOPATHY
4. CVS :
https://60shirisha.blogspot.com/2021/06/medicine-case-discussion_14.html?m=1
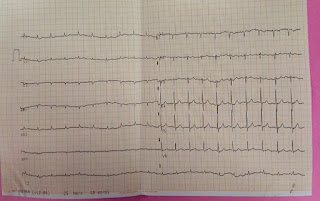
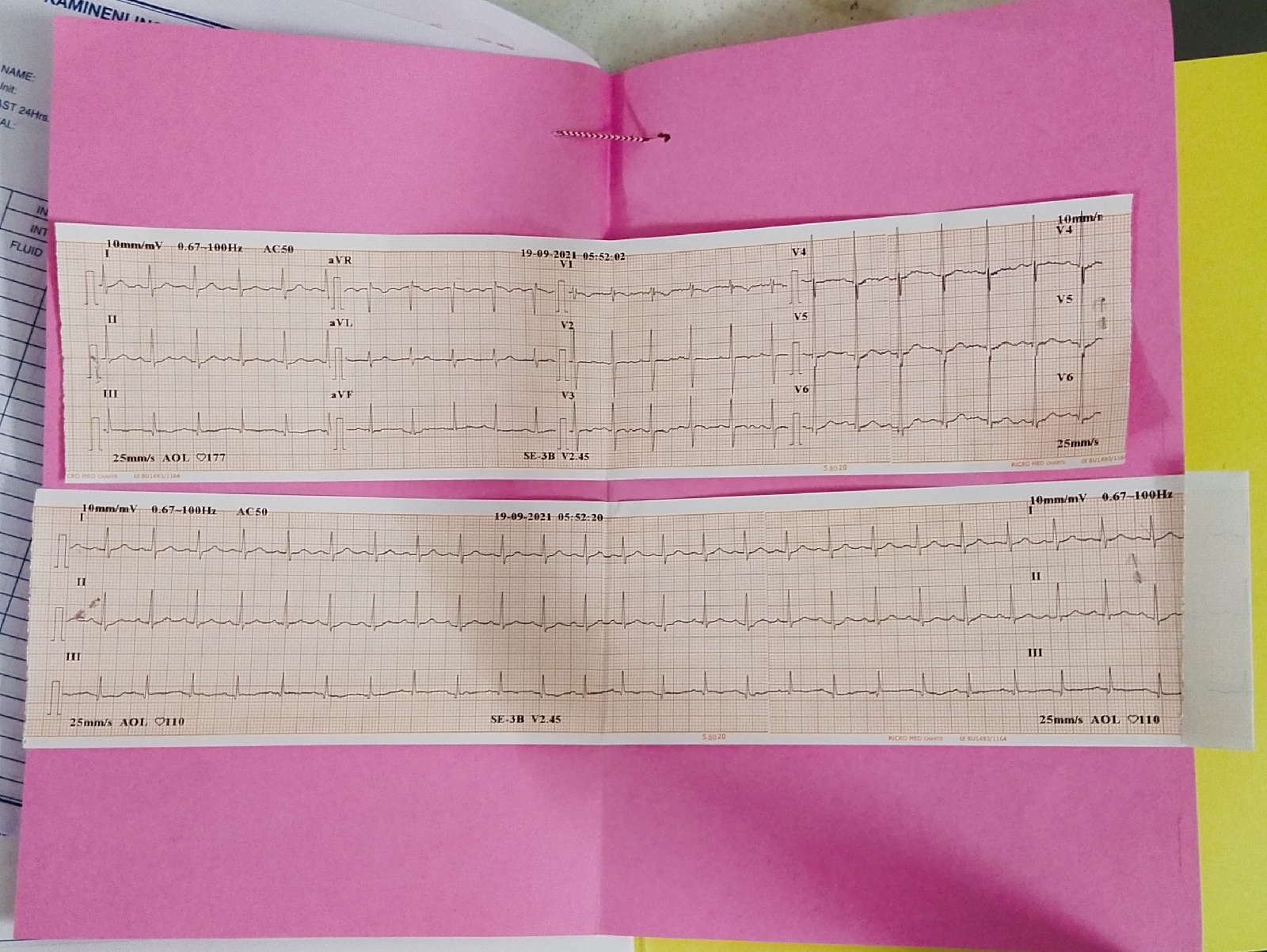
OVERVIEW:-A 70 year old with complaints of Distension of abdomen and shortness of breath Grade-3 since 5days with ECG Showing Atrial fibrillation
And 2D Echo ;
Akinetic segment in LAD territory with EF 35% and RVSP 100mmhg
B/L pleural effusion,mild pericardial effusion.
Diagnosed as
HFrEF with Atrial fibrillation 2 to ?IHD
Her biochemical report showing severe hyperthyroidism possibly relating to her refractory Atrial fibrillation
APPRAISAL:-well
Presented case with history and detailed findings in ECG and 2D ECHO
NEGATIVES:-Could have shared the BP CHARTING AND FEVER CHARTING with deidentified clinical
Images of patient.
ANALYSIS:-A 70 year old with complaints of Distension of abdomen and shortness of breath Grade-3 since 5days with ECG Showing Atrial fibrillation investigations showing
HFrEF with Atrial fibrillation 2 to ?IHD
And Her biochemical report showing severe hyperthyroidism possibly relating to her refractory Atrial fibrillation
Q2) Share the link to your own case report of a patient that you connected with and engaged while capturing his her sequential life events before and after the illness and clinical and investigational images along with your discussion of that case.
http://krupalatha54.blogspot.com/2021/06/is-online-e-log-book-to-discuss-our.html
Q 5) Testing scholarship competency in
logging reflective observations on your concrete experiences of this last month : (10 marks)
Reflective logging of one's own experiences is a vital tool toward competency development in medical education and research.
THIS POSTING HAS BEEN A LEARNING EXPERIENCE ON ANALYSING THE LOGGING THE PATIENT DATA AND GETTING TO KNOW ABOUT THE TREATMENT PROTOCOL
AND HANDS ON EXPOSURE REGARDING RYLES TUBE AND FOLEYS CATHETER INSERTION
PERFORMING DIALYSIS SESSIONS
PRESENTING THE CASES IN 2-4 sessions
Comments
Post a Comment